Owing largely to the “French Paradox,” wine—particularly red wine—was long considered the alcoholic beverage most likely to impart significant health benefits. This idea has permeated academic research, food and beverage marketing, and the popular press. Our purpose is not to dispel the notion that moderate wine consumption has health benefits but rather to discuss the growing literature on the health benefits of beer, which is comparable to wine in many respects, but not popularly viewed as a healthy choice.
This article synthesizes and discusses the research that may inform updated and more nuanced recommendations on beer consumption and health on the part of the federal government. There is also the potential to inform policy on alcohol sales, taxation, and consumption. For example, federal, state, and local governments have laws and regulations in place regarding the allowable alcohol-by-volume (ABV), distribution limits, techniques for manufacturing alcohol, and allowable container types. Most of these laws are intended to curb unhealthy and binge drinking, but they are debatably effective. There is certainly precedent for government regulation with respect to beer consumption by type and likely room for the laws to be improved and refined and educational efforts to be put in place.
Before we dive into the potential benefits of moderate beer consumption, we must emphasize that this discussion centers on moderate consumption. There is no question that alcohol is an addiction for some individuals and alcoholism is very costly, both for society and for the individual. A wealth of literature examines the underpinnings of addiction (see Gilpin and Koob, 2008, for a discussion of the neurobiology of dependence) and some individuals may be better off not drinking at all. Furthermore, we stress that the inclusion of moderate alcohol in a healthy diet is not a substitute for foods such as fruits and vegetables.
Researchers in nutrition, epidemiology, and the social sciences have been studying the health impacts of alcohol consumption for decades. Empirical research across disciplines find the relationship between alcohol consumption and health to be “U-shaped” or “J-shaped.” For example, Marmot et al. (1981) was one of the earliest studies to illustrate this phenomenon explicitly, studying the alcohol intake and mortality of 1,422 men over 10 years. The authors found that moderate drinking (less than 34 grams of alcohol per day, the equivalent of 2.4 alcoholic drinks, defined in detail below), was associated with a decreased risk of mortality relative to both heavy drinking and not drinking at all. Since that time, studies have shown moderate alcohol intake to have protective effects with respect to cardiovascular disease (Marmot and Brunner, 1991), stroke (Berger et al., 1999), type-2 diabetes (Baliunas et al., 2009), cancer (Tsugane et al., 1999), and other ailments.
Originally, much of the discussion regarding the purported health benefits of alcohol consumption revolved around the so-called “French Paradox.” Among developed countries, the French have low rates of chronic heart disease relative to their per capita consumption of saturated fats. In an influential study, Renaud and de Lorgeril (1992) argued that moderate alcohol consumption reduces blood platelet aggregation, thereby reducing the risk of heart disease and helping resolve the “paradox.” A wealth of studies and literature reviews since that time (Bertelli and Das, 2009) has discussed the protective effects of resveratrol, an antioxidant found in wine grapes. It is due to this research, in part, that wine is often noted to be the most healthful alcoholic beverage, when consumed in moderation (Gronbaek et al., 1995).
However, the research on alcohol and health continues to evolve and evidence is mounting that beer has its own health-protective attributes and effects. Notably, beer contains xanthohumol, a flavonoid found in hops, one the key ingredients in the beer-brewing process. Xanthohumol has been shown to inhibit cancer growth at the cellular level (Vanhoecke et al., 2005) and to impart health impacts through the mechanism of beer drinking (Magalhaes et al., 2009). Beer also contains a number of nutrients not found in wine or spirits, including fiber, minerals, and B vitamins (Denke, 2000; Bamforth, 2002).
Keil et al. (1997) and Brenner et al. (2001) both demonstrated the familiar health impacts of moderate alcohol consumption on predominantly beer-drinking populations. The former study identified a U-shaped curve between alcohol consumption, mostly beer, and both coronary heart disease and mortality. The lowest health risks were associated with men drinking between 20 and 39.9 grams of alcohol per day (approximately 1.43 to 2.85 drink equivalents). The latter study found a significant inverse relationship between alcohol drinking, again mostly beer, and coronary heart disease among adult German men. Burger and Mensink (2004) also studied the German population using the National Health Interview and Examination Survey, which combines dietary recall data with health outcomes. The authors calculated total upper alcohol limits, or daily consumption levels up to which no significant harmful health affects occur with drinking, of 20–24 grams/day for men (1.43–1.71 equivalent drinks) and 10–12 grams/day for women (0.71–0.86 equivalent drinks).
Many additional health benefits specific to beer have been identified using longitudinal data. Wannamethee et al. (2004) found a strong inverse relationship between alcohol consumption and weight gain among women over an eight-year period, with the effects of beer drinking comparable in magnitude to those of wine drinking. Thadhani et al. (2002) identified a reduced risk of hypertension associated with light beer drinking among younger women. The authors noted that both wine and beer demonstrate significant health impacts, though the wine effect seems to be larger in magnitude across studies. Wannamethee et al. (2003) demonstrated an inverse relationship between alcohol consumption and type-2 diabetes among women drinking wine and beer but not spirits. The extracts from hops and yeast, when drunk via beer, have been shown to impart skin health and even hasten the healing process of wounds in laboratory experiments (Chen et al., 2014). In yet another example, Pedrera-Zamorano et al. (2009) demonstrated the potential of beer drinking to increase bone mass in adult women.
A number of studies have compared the health effects of beer to other alcohol types directly. One of the earliest studies to do so was Hennekens et al. (1979), who found that moderate beer drinking reduced the risk of coronary heart disease even more than drinking wine or liquor. However, for all types of alcohol, consumption above 59.2 ml per day was associated with increased risks. In a large-scale meta-analysis, Di Castelnuovo et al. (2002) analyzed the impacts of beer and wine drinking on cardiovascular health risks. More recently, Volpe et al. (2016) used household scanner data and self-reported health outcomes to demonstrate that beer consumption has comparable protective effects to wine with respect to coronary heart disease and type-2 diabetes.
The potential associations between alcohol consumption and dementia and cognitive decline have also been examined extensively. Peters et al. (2008) reviewed 23 studies on the topic and concluded that light to moderate alcohol drinking likely has protective effects against dementia late in life. Beer is unique among alcoholic beverages in that it contains silicon. Gonzalez-Munoz et al. (2008) note that beer may have additional benefits for preventing Alzheimer’s Disease, as silicon has been shown to prevent the absorption of aluminum, one of the likely contributing factors to the ailment.
The Dietary Guidelines for Americans, issued jointly by U.S. Department of Agriculture and Department of Health and Human Services, are intended to summarize the extant research on nutrition and biology in order to inform Americans about healthy eating habits. The 2015–2020 edition of the Dietary Guidelines addresses alcohol as follows:
Regarding alcohol, the Committee confirmed several conclusions of the 2010 DGAC, including that moderate alcohol intake can be a component of a healthy dietary pattern, and that if alcohol is consumed, it should be consumed in moderation and only by adults.
A major change in the Dietary Guidelines from the last edition is how much alcohol is contained in a “standard” drink. Various trade associations voiced concern that the previous definition of a standard alcoholic drink was too vague and that consumers could potentially assume a martini and a pint of beer to have the same alcoholic content. Table A9–1 of the 2015 Dietary Guidelines shows the basic calculation for determining the number of standard drinks in an alcoholic beverage:
One alcoholic drink is defined as containing 14 grams (0.6 fl oz) of pure alcohol… To calculate drink-equivalents, multiply the volume in ounces by the alcohol content in percent and divide by 0.6 ounces of alcohol per drink-equivalent. For example: 16 fl oz beer at 5% alcohol: (16 fl oz)(0.05)/0.6 fl oz = 1.3 drink-equivalents.
The Dietary Guidelines, however, do not address any of the health effect differences across types of alcoholic beverages. Moreover, research suggests that the health effects of moderate alcohol consumption may depend on factors such as age or gender, neither of which are addressed in the Dietary Guidelines comments on alcohol. Furthermore, without a clear discussion of healthful and unhealthful consumption, there is the potential for individuals to misinterpret the current body of research.
Despite the extensive body of evidence supporting moderate beer drinking as a component of a healthy diet and lifestyle, there are risks associated with alcohol consumption. Such risks should also be taken into account in dietary recommendations and regulations. Most, though not all, studies identifying inverse relationships between alcohol consumption and risk factors for ailments have found that high or excessive alcohol consumption is harmful to health and longevity. This is consistent with the familiar U-shaped curve. Corroborating the health and societal risks of excessive drinking, the Centers for Disease Control estimates that the annual cost of alcohol abuse is about $223 billion. This includes medical and legal costs, among other damages, 75% of which can be attributed to binge drinking.
We argue that perhaps the most important cautionary guideline regarding beer consumption and health is to avoid binge drinking. The National Institute on Alcohol Abuse and Alcoholism defines binge drinking as that which raises the blood alcohol content above 0.08. This typically translates into five drinks within two hours for men, four for women. They further summarize national health surveys indicating that 70% of binge drinking episodes involve adults 26 years and older, even though 90% of alcohol consumed by youth under the age of 21 is in the form of binge drinking. Furthermore, binge drinkers are 14 times more likely to report alcohol-impaired driving than non-binge drinkers, binge drinking is more prevalent among men than women, and more than half of alcohol consumed in the United States is in the form of binge drinking.
According to the World Health Organization (WHO) (2014) on per capita annual alcohol consumption for individuals 15 and older, each individual in the United States consumed 4.16 liters of pure alcohol in beer in 2010. Using the Dietary Guidelines’ conversion to standard drinks, this equates to 0.64 drinks per day. Some studies have suggested that moderate alcohol consumption may include at least one day a week of non-drinking (Anderson, 1996). If we then average the quantity of alcohol consumed over a six-day drinking week, the average number of beers consumed by all Americans per day is 0.75.
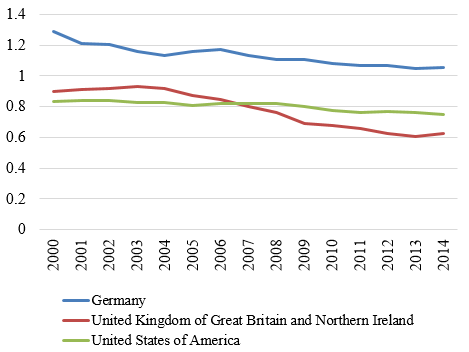
Source: World Health Organization (WHO, 2017).
We know, however, that not all of the population over the age of 15 drinks. According to the 2015 National Survey on Drug Use and Health (SAMHSA, 2015), 70.1% of people ages 18 or older reported drinking in the past year. Adjusting the WHO alcohol consumption statistics to this drinking population, average annual beer consumption becomes roughly 1.07 drinks per day for a six-day drinking week, well below the definition of moderate alcohol consumption. Figure 1 compares the number of alcoholic drink equivalents in the United States to the United Kingdom and Germany (comparable drinking countries where binge drinking is considered a serious social problem) for a six-day drinking week. Note that per capita beer consumption has been decreasing in each country and, in all cases, falls below moderate consumption levels.
Given the average amount of beer consumed in the United States and the prevalence of binge drinking, we can conclude that the major issue of unhealthy consumption is not related to total quantity of alcohol consumed but the timing of consumption. It stands to reason then that efforts toward education should emphasize what healthy consumption is and is not and the benefits of beer as a component of a healthy diet and lifestyle. Current guidelines and educational efforts could therefore be improved to highlight the benefits of beer, relative to spirits or malt beverages for example, and to further caution against the practice of binge drinking.
So, what is healthy consumption of beer? Given all that we have observed from previous studies, unhealthy consumption is clear. However, it appears that there exists a need to educate Americans on how beer can be incorporated into a healthy diet. Adjusting the culture of beer consumption away from binge drinking could drastically reduce the economic burden of unhealthy consumption. Private efforts are being made to try to do this, but these may be misleading without a clear discussion of the healthy components of beer, via the Dietary Guidelines.
An example is the proposal for nutrition labeling of major beer brands. Anheuser-Busch InBev, Molson Coors, Constellation Brands, and Heineken have all agreed to provide nutrition facts on labels by 2020. These will include serving size, servings per container, calories, carbohydrates, protein, and fat content. Nutrition fact labels will not, however, educate consumers on how different beers have different ingredients that may contain more beneficial vitamins and minerals then others. For instance, niacin (vitamin B3) has been shown to significantly increase HDL cholesterol and reduce LDL cholesterol. Depending on the major ingredients of the beer—rice or malted barley or residual brewer’s yeast after filtration—the amount of beneficial niacin can drastically differ. Just as the Dietary Guidelines discuss the different components of beneficial ingredients contained in foods such as animal protein and their relationship to a healthy diet in moderation, there is a possibility to do so with beer and all alcoholic beverages.
Moreover, we argue that some current state and local alcohol policy (such as restrictions to access) may incentivize unhealthy drinking behavior. As an extreme example, take early 20th century common law in Australia and New Zealand, which required pubs to close at 6pm. This requirement led to what became known as the “Six O’clock Swill,” a period of excessive binge drinking between the end of the workday and closing time. Across the United States today, various laws prohibit the sale of alcohol on certain days of the week. Research has suggested that these laws do not affect total alcohol consumption as much as the timing of consumption. For example, Carpenter and Eisenberg (2009) showed that repealing a Sunday alcohol sales ban in Canada resulted in consumers shifting some of their Saturday consumption to Sundays. The ban may actually have promoted binge drinking among certain consumers. Understanding that total beer consumption on average is below what is considered a moderate amount and that there are significant health benefits to moderate consumption should help better inform policy and avoid restrictive policy with unintended consequences.
Anderson, P. 1996. “Guidelines on Sensible Drinking.” Addiction 91(1):25–33.
Baliunas, D.O., B.J. Taylor, H. Irving, M. Roerecke, J. Patra, S. Mohapatra, and J. Rehm. 2009. “Alcohol as a Risk Factor for Type 2 Diabetes.” Diabetes Care 32(11):2123–2132.
Bamforth, C. 2002. “Nutritional Aspects of Beer – A Review.” Nutrition Research 22(1–2):227–237.
Bertelli, A.A., and D.K. Das. 2009. “Grapes, Wines, Resveratrol, and Heart Health.” Journal of Cardiovascular Pharmacology 54(6):468–476.
Berger, K., U.A. Ajani, C.S. Kase, J.M. Gaziano, J.E. Buring, R.J. Glynn, and C.H. Hennekens. 1999. “Light-to-Moderate Alcohol Consumption and the Risk of Stroke among US Male Physicians.” New England Journal of Medicine 341(21):1557–1564.
Brenner, H., D. Rothenbacher, G. Bode, W. März, A. Hoffmeister, and W. Koenig. 2001. “Coronary Heart Disease Risk Reduction in a Predominantly Beer-Drinking Population.” Epidemiology 12(4):390–395.
Burger, M., and G.B. Mensink. 2004. “High Alcohol Consumption in Germany: Results of the German National Health Interview and Examination Survey 1998.” Public Health Nutrition 7(07):879–884.
Carpenter, C.S., and D. Eisenberg. 2009. “Effects of Sunday Sales Restrictions on Overall and Day-Specific Alcohol Consumption: Evidence from Canada.” Journal of Studies on Alcohol and Drugs 70(1):126–133.
Chen, W., T. Becker, F. Qian, and J. Ring. 2014. “Beer and Beer Compounds: Physiological Effects on Skin Health.” Journal of the European Academy of Dermatology and Venereology 28:142–150.
Centers for Disease Control and Prevention. 2014. Excessive Drinking Costs U.S. $223.5 Billion. Available online: https://www.cdc.gov/features/alcoholconsumption/
Denke, M.A. 2000. “Nutritional and Health Benefits of Beer.” American Journal of the Medical Sciences 320(5):320–326.
Di Castelnuovo, A., S. Rotondo, L. Iacoviello, M.B. Donati, and G. de Gaetano. 2002. “Meta-analysis of Wine and Beer Consumption in Relation to Vascular Risk.” Circulation 105(24):2836–2844.
Gilpin, N.W., and G.F. Koob. 2008. “Neurobiology of Alcohol Dependence: Focus on Motivational Mechanisms.” Alcohol Research and Health 31(3):185–195.
González-Muñoz, M.J., A. Pena, and I. Meseguer. 2008. “Role of Beer as a Possible Protective Factor in Preventing Alzheimer’s Disease.” Food and Chemical Toxicology 46(1):49–56.
Gronbaek, M., A. Deis, T.I. Sorensen, U. Becker, P. Schnohr, and G. Jensen. 1995. “Mortality Associated with Moderate Intakes of Wine, Beer, or Spirits.” British Medical Journal 310(6988):1165–1169.
Hennekens, C.H., W. Willett, B. Rosner, D.S. Cole, and S.L. Mayrent. 1979. Effects of Beer, Wine, and Liquor in Coronary Deaths. JAMA 242(18): 1973-1974.
Keil, U., L.E. Chambless, A. Doring, B. Filipiak, and J. Stieber. 1997. “The Relation of Alcohol Intake to Coronary Heart Disease and All-Cause Mortality in a Beer-Drinking Population.” Epidemiology 8(2):150–156.
Magalhaes, P.J., D.O. Carvalho, J.M. Cruz, and A.A. Barros. 2009. “Fundamentals and Health Benefits of Xanthohumol, a Natural Product Derived from Hops and Beer.” Natural Product Communications 4(5):591–610.
Marmot, M.G., M.J. Shipley, G. Rose, and B.J. Thomas. 1981. “Alcohol and Mortality: A u-Shaped Curve.” Lancet 317(8220):580–583.
Marmot, M., and E. Brunner. 1991. “Alcohol and Cardiovascular Disease: The Status of the U Shaped Curve.” British Medical Journal 303(6802):565–568.
National Institute on Alcohol Abuse and Alcoholism. 2016. Drinking Levels Defined. Available online: http://www.niaaa.nih.gov/alcohol-health/overview-alcohol-consumption/moderate-binge-drinking
Pedrera-Zamorano, J.D., J.M. Lavado-Garcia, R. Roncero-Martin, J.F, Calderon-Garcia, T. Rodriguez-Dominguez, and M.L. Canal-Macias. 2009. “Effect of Beer Drinking on Ultrasound Bone Mass in Women.” Nutrition 25(10):1057–1063.
Peters, R., J. Peters, J. Warner, N. Beckett, and C. Bulpitt. 2008. “Alcohol, Dementia and Cognitive Decline in the Elderly: A Systematic Review.” Age and Ageing 37(5):505–512.
Renaud, S.D., and M. de Lorgeril. 1992. “Wine, Alcohol, Platelets, and the French Paradox for Coronary Heart Disease.” The Lancet 339(8808):1523-1526.
Substance Abuse and Mental Health Services Administration (SAMHSA). 2015. National Survey on Drug Use and Health (NSDUH). Table 2.41B—Alcohol Use in Lifetime, Past Year, and Past Month among Persons Aged 12 or Older, by Demographic Characteristics: Percentages, 2014 and 2015. Available online: https://www.samhsa.gov/data/sites/default/files/NSDUH-DetTabs-2015/NSDUH-DetTabs-2015/NSDUH-DetTabs-2015.htm#tab2-41b
Thadhani, R., C.A. Camargo, M.J. Stampfer, G.C. Curhan, W.C. Willett, and E.B. Rimm. 2002. “Prospective Study of Moderate Alcohol Consumption and Risk of Hypertension in Young Women.” Archives of Internal Medicine 162(5):569–574.
Tsugane, S., S. Sasaki, S. Baba, and JPHC Study Group. 1999. “Alcohol Consumption and All-Cause and Cancer Mortality among Middle-Aged Japanese Men: Seven-Year Follow-Up of the JPHC Study Cohort I.” American Journal of Epidemiology 150(11):1201–1207.
U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2015. 2015 – 2020 Dietary Guidelines for Americans, 8th ed. Available online: http://health.gov/dietaryguidelines/2015/guidelines/
Vanhoecke, B., L. Derycke, V. Van Marck, H. Depypere, D. De Keukeleire, and M. Brackem. 2005. “Antiinvasive Effect of Xanthohumol, a Prenylated Chalcone Present in Hops and Beer.” International Journal of Cancer 117(6):889–895.
Volpe, R., M. McCullough, M.K. Adjemian, and T. Park. 2016. “Beer-Purchasing Behavior, Dietary Quality, and Health Outcomes among US Adults.” Journal of Wine Economics 11(03):436–464.
Wannamethee, S.G., C.A. Camargo, J.E. Manson, W.C. Willett, and E.B. Rimm. 2003. “Alcohol Drinking Patterns and Risk of Type 2 Diabetes Mellitus among Younger Women.” Archives of Internal Medicine 163(11):1329–1336.
Wannamethee, S.G., A.E. Field, G.A. Colditz, and E.B. Rimm. 2004. “Alcohol Intake and 8†Year Weight Gain in Women: A Prospective Study.” Obesity Research 12(9):1386–1396.
World Health Organization. 2017. “WHO Country Profiles: United States of America.” Available online at: http://www.who.int/substance_abuse/publications/global_alcohol_report/profiles/usa.pdf?ua=1

