The global obesity epidemic may have finally met its match in a novel class of medications that include brand names such as Ozempic, Wegovy, and Zepbound (Cousin-Frankel, 2023). While initially introduced as a treatment for type-2 diabetes, patients taking glucagon-like peptide 1 (GLP-1) receptor agonists (see Text Box 1) found a discrete change in the amount and types of food they desire, including the curbing of cravings for certain less nutritious categories of foods (e.g., sweets, fried foods), which helped patients who were overweight or obese lose clinically significant amounts of weight and, with continued use, to maintain weights 15%–20% lower than premedication levels (Rubino et al., 2021, Aronne et al., 2024).
The change in food consumption after weight loss can be eye-opening. Consumers on these medications eat less food, both during the period when weight is declining and once a new, lower weight is achieved. An individual in a normal weight range consumes about 280 fewer pounds of food per year compared to someone who is obese (Body Mass Index or BMI of 30 or higher) and about 139 pounds less relative to an individual in the overweight range (BMI between 25 and 30) (Serafini and Toti, 2016). Not only does the amount of food consumed decline, but early indications suggest that the types of food preferred by those on anti-obesity medications also changes (Bettadapura et al., 2024).
|
Glucagon-like peptide 1 (GLP-1) receptor agonists are a key ingredient of a novel class of medications that help many patients achieve clinically significant weight loss. GLP-1 is a hormone generated in the small intestine that has several roles that can shape the amount of food that humans might demand, including lowering blood sugar levels, slowing the emptying of the stomach, and signaling fullness to the brain. These drugs operate as an agonist to the GLP-1 receptor, effectively allowing more of the hormone to remain in circulation. This class of drugs include liraglutide (sold under brand names including Saxenda, Victoza), semaglutide (Ozempic, Wegovy, Rybelsus), and tirzepatide (Zepbound and Monjaro). These drugs are synthesized, often with the help of re-engineered yeast cells (Xu et al., 2017), and the first injectable drug was prescribed in 2005 for patients with Type-II diabetes (Gribble and Reimann, 2021). The discovery timeline for this class of drugs includes inspiration drawn from chemicals identified in the saliva of the Gila monster (Diabetes in Control, 2007). As of 2024, nine different companies have at least 18 formulations in the drug development and approval pipeline (Collins et al., 2024) as large pharmaceuticals vie for what is projected to be a more than a $150 billion global market by 2031 (Economist, 2024). |
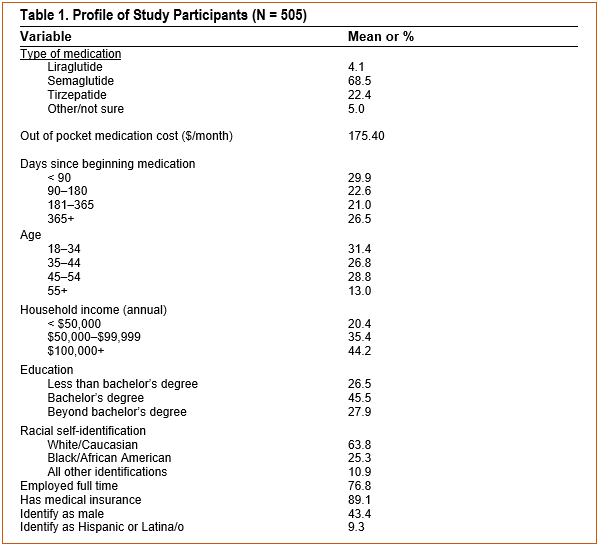
In April 2024, 505 U.S. consumers who reported current use of one of these drugs described how their foodconsumption and spending habits had changed since beginning the GLP-1 medication (see Table 1 for a profile of study participants and Mansouri and Roe, 2024, and Roe, 2024, for details of the study). Key insights from this study are summarized and discussed below.
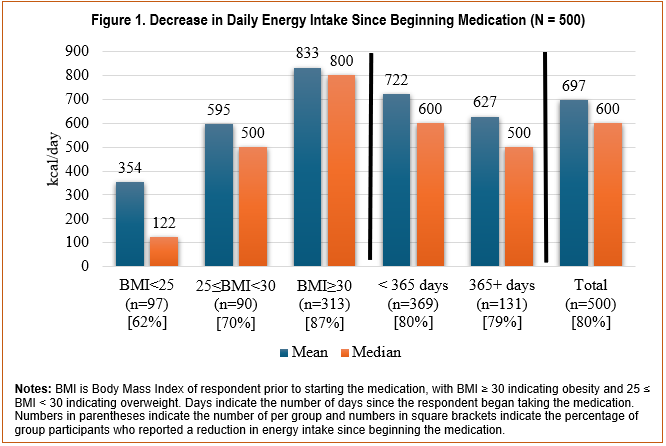
The average respondent decreased daily energy intake by nearly 700 kcals (22%) compared to before starting the medication with 80% reporting at least some calorie reduction (Figure 1). Considering that only those whohad a BMI of 30 or more prior to beginning medication (i.e., those with obesity who might be most likely to begin such medications if insurers expand coverage), the average post-medication calorie reduction increases to 833 kcal/day (26%). However, even those with premedication BMIs under 25 (not classified as either overweight or obese and presumably prescribed the medication for purposes of controlling type-2 diabetes) reported an average daily energy reduction of 354 kcals/day (14%). The daily calorie reduction is about 100 kcal/day less among those who have been on the medication for more than a year versus less than a year, though that difference is not statistically significant (p = 0.31) and the percentage reduction remains sizable (26%).
Eating less also translates to spending less on food. Of the respondents who provided estimates of their current and premedication spending on food and drink, the median reduction in weekly spending on groceries and other food for home consumption was $10 (about 11%), on food away from home was $30 (about 29%), and on alcohol was $1 (7%). Another source of savings may arise from wasting less of the food that is purchased. When asked if they are wasting more food since beginning the medication, 25% agreed, while 61% disagreed (Mansouri and Roe, 2024). The amount of food that patients waste declines, particularly as patients become more familiar with the medication, if patients do not suffer common side effects like nausea, and if they switch their dietary patterns to focus more on fruits and vegetables (Mansouri and Roe, 2024).
While spending on food and drink declined, 87% of respondents had to spend at least some of their own money to obtain the GLP-1 medication. The median respondent reported spending $60/month out of their own pocket to obtain the medication, while the sample average was $175.40/month. About 61% of the sample saved more money on food and drink than they spent to obtain the medication, with the median monthly savings of $145.77. While changes in other types of spending were not reported in detail, about 86% reported at least one side effect from taking the drug (nausea and constipation were most frequent), and 29% agreed that they spent more money on medications to treat side effects.
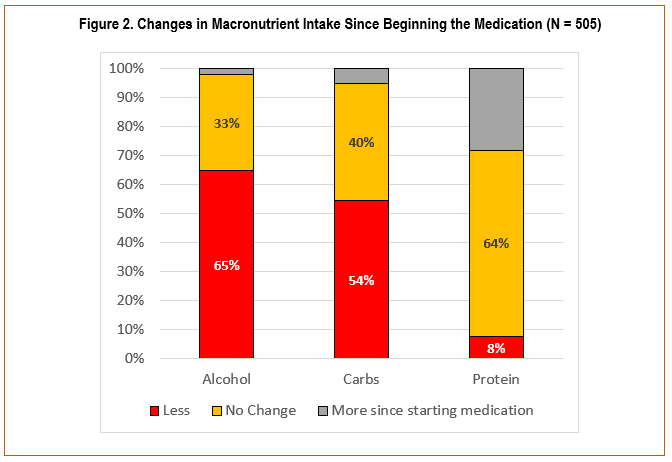
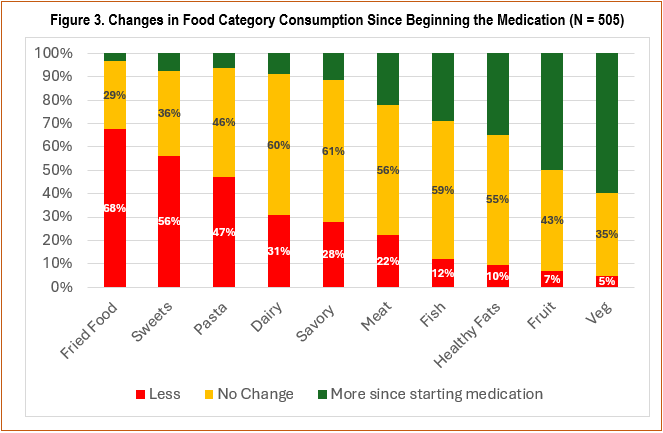
About 75% of respondents agreed that the types of foods they eat had changed since beginning the medication. Among broad-based calorie sources (Figure 2), more respondents reported consuming less alcohol (65%) and carbohydrates (40%). Few reported eating less protein (8%), while 28% reported increasing protein consumption since beginning the medication. Drilling down into narrower food categories (Figure 3), fried foods (68%), sweets (56%), pasta (47%) and dairy (31%) were the most likely to be consumed less since starting the medication.
Foods most likely to be consumed more since beginning the medication include vegetables (60%), fruit (50%), healthy fats (35%) and fish (29%). Meat was the one category that was equally balanced, with 22% of respondents reporting increased consumption, 22% reporting decreased consumption, and the remainder reporting no change since beginning the medication. Respondents were not asked if the change in food preferences was due to medical advice received as part of their prescription or if it was simply a result of taking the medication, a question that would be important to ask in future studies to understand the malleability of food changes to medical advice.
Similar shifts in food preferences have also been noted by others. For example, previous studies have noted a decrease in preference for starchy foods (Wharton et al., 2022), dairy (Friedrichsen et al., 2021, Wharton et al., 2022), sweets (Friedrichsen et al., 2021, Kadouh et al., 2020, Gibbons et al., 2021), savory foods (Friedrichsen et al., 2021, Kadouh et al., 2020), and high-fat foods (Blundell et al., 2017, Gibbons et al., 2021, Kadouh et al., 2020). Industry has already recognized the potential for disruption of normal food formulation and marketing practices (Peck, 2023), with at least one firm having already developed a food product line tailored to the perceived needs of medication users (Back, 2024).
Nearly 3 billion people around the world were considered overweight or obese in 2022, including one in eight adults who were classified as obese (WHO, 2024). In theUnited States, 41% of adults are estimated to be obese, with an additional 32% estimated to be overweight (Hales et al., 2020). As of May 2024, about 6% of U.S. adults reported taking a GLP-1 drug, with about 38% of those (about 2.3% total) taking the drug to address excess weight (Montero et al., 2024). Further, about 60% said they think Medicare should cover the cost of these drugs when prescribed to address overweight and obesity, with this support largely uniform across partisan political affiliations (Montero et al. 2024).
While current supplies of these novel medications are limited due to production bottlenecks (Lipanovic, 2024), one might expect a decrease in patient out-of-pocket costs due to expansion of production capacity (Novo Nordisk, 2024), increased market competition (Liu et al., 2021, Collins et al., 2024), expanded insurance coverage (Liu and Rome, 2024, Cubanski and Neuman, 2024), and, eventually, expiration of patent protections (Alhiary et al., 2023). Insurance coverage may be the biggest influence on the uptake of GLP-1 medications over the next few years.
Insurance companies are expecting high levels of consumer cost sharing (Kim, Hwang, and Fendrick, 2024), while other insurers have limited the amount of time that a patient can receive coverage while on a GLP-1. Nationwide, high out-of-pocket (OOP) drug costs have impeded access to GLP-1 medications for many people. A single month’s worth of maintenance dosing for GLP-1 medication costs on average $1,305.37 (Docimo et al., 2024). While Medicare Part D plans can cover drugs like Wegovy for patients who have obesity-related conditions like diabetes or to cut cardiovascular risks among patients who are obese (Cubanski and Neuman, 2024), a broader debate is evolving about whether public and private insurers should cover these medications to reduce obesity even if patients are not yet suffering any medical conditions associated with excess weight (Wreschnig, 2024, Ward et al., 2023, Hernandez et al., 2023). A growing number of employers and health plans in the United States have eliminated coverage of anti-obesity medications due to the increase in the number of patients being prescribed the medication (Robbins, 2024).
Studies also suggest patients on these medications face a lower risk of death from all causes (Lincoff et al., 2023), are less likely to suffer opioid overdoses (Qeadan, McCunn, and Tingey, 2024), were less likely to die after getting COVID (Scirica et al., 2024), and incur fewer nonmedication healthcare costs (Watkins et al., 2022). Further, studies of medium-term term usage (4–7 years) are not revealing unexpected adverse effects beyond those typically experienced among patients in drug trials (Lincoff et al., 2023, Courtney et al., 2017).
Many of these evolving factors suggest that GLP-1 drugs will become a growing part of the American and global medical landscape moving forward and should be factored into projections of national and global fooddemand. For example, if the median caloric intake and spending reductions reported by respondents in thisstudy were to hold moving forward, and uptake to address overweight and obesity were to increase to more moderate levels in the United States—say to 10% among the overweight and to 20% among adults who are obese—it would suggest a 3% reduction in total caloric demand. This translates to about 20 billion fewer calories of food consumed each day and about $1.2 billion less spent per week on food and drink in the United States, with a disproportionate amount of these reductions accruing to those producing alcoholic beverages, carbohydrates, sweets, and dairy, while those producing and marketing vegetables, fruit, healthy fats and fish may see little to no decline. Much more work is required to fully understand how GLP-1 medications will translate to food system and farm level impacts, however, including improving data collection about the dietary habits of those newly introduced to the medication and the patterns of adherence to prescribed medications will be foundational to these efforts.
Alhiary, R., A.S. Kesselheim, S. Gabriele, R.F. Beall, S.S. Tu, Sand W.B. Feldman. 2023. “Patents and Regulatory Exclusivities on GLP-1 Receptor Agonists.” JAMA 330(7):650–657.
Aronne L.J., N. Sattar, D.B. Horn, H.E. Bays, S. Wharton, W.Y. Lin, N.N. Ahmad, S. Zhang, R. Liao, M.C. Bunck, and I. Jouravskaya. 2024. “Continued Treatment with Tirzepatide for Maintenance of Weight Reduction in Adults with Obesity: The SURMOUNT-4 Randomized Clinical Trial.” JAMA 331(1):38–48.
Back, A. 2024. “Big Food Is Learning to Love Weight-Loss Drugs.” Wall Street Journal, October 25. Available online: https://www.wsj.com/health/pharma/glp-1-weight-loss-drugs-food-industry-opportunities-8e375102.
Bettadapura, S., K. Dowling, K. Jablon, A.W. Al-Humadi, and C.W. le Roux. 2024. “Changes in Food Preferences and Ingestive Behaviors after Glucagon-Like Peptide-1 Analog Treatment: Techniques and Opportunities.” International Journal of Obesity 1–9.
Blundell, J., G. Finlayson, M. Axelsen, A. Flint, C. Gibbons, T. Kvist, and J.B. Hjerpsted. 2017. “Effects of Once‐Weekly Semaglutide on Appetite, Energy Intake, Control of Eating, Food Preference and Body Weight in Subjects with Obesity.” Diabetes, Obesity and Metabolism 19(9):1242–1251.
Collins, E., A. Beattie, S.V. Ramagopalan, and J. Pearson-Stuttard. 2024. “First in Class, Best in Class or a Wild Card: Who Will Dominate the Anti-Obesity Medication Market?” Journal of Comparative Effectiveness Research 13(7):e240044.
Courtney, H., R. Nayar, C. Rajeswaran, and R. Jandhyala. 2017. “Long-Term Management of Type 2 Diabetes with Glucagon-Like Peptide-1 Receptor Agonists.” Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy 10:79–87.
Couzin-Frankel, J. 2023. “Obesity Meets Its Match.” Science 382:1226–1227.
Cubanski, J., and T. Neumann. 2024. “Medicare Spending on Ozempic and Other GLP-1s Is Skyrocketing.” Kaiser Family Foundation, March 22. Available online at: https://www.kff.org/policy-watch/medicare-spending-on-ozempic-and-other-glp-1s-is-skyrocketing/ [Accessed September 7, 2024].
Diabetesincontrol.com. 2007. “Dr. John Eng’s Research Found That the Saliva of the Gila Monster Contains a Hormone That Treats Diabetes Better Than Any Other Medicine.” Available online: https://www.diabetesincontrol.com/dr-john-engs-research-found-that-the-saliva-of-the-gila-monster-contains-a-hormone-that-treats-diabetes-better-than-any-other-medicine/ [Accessed November 8, 2024].
Docimo, S., J. Shah, G. Warren, S. Ganam, J. Sujka, and C. DuCoin. 2024. “A Cost Comparison of GLP-1 Receptor Agonists and Bariatric Surgery: What Is the Break Even Point?” Surgical Endoscopy 38(11):6560–6565.
The Economist. 2024. “GLP-1s Like Ozempic Are among the Most Important Drug Breakthroughs Ever.” October 24. Available online: https://www.economist.com/briefing/2024/10/24/glp-1s-like-ozempic-are-among-the-most-important-drug-breakthroughs-ever
Friedrichsen, M., A. Breitschaft, S. Tadayon, A. Wizert, and D. Skovgaard. 2021. “The Effect of Semaglutide 2.4 mg Once Weekly on Energy Intake, Appetite, Control of Eating, and Gastric Emptying in Adults with Obesity.” Diabetes, Obesity and Metabolism 23(3):754–762.
Gibbons C., J. Blundell, S. Tetens Hoff, K. Dahl, R. Bauer, and T. Baekdal. 2021. “Effects of Oral Semaglutide on Energy Intake, Food Preference, Appetite, Control of Eating and Body Weight in Subjects with Type 2 Diabetes.” Diabetes, Obesity and Metabolism 23:581–588.
Gribble, F.M., and F. Reimann. 2021. “Metabolic Messengers: Glucagon-like Peptide 1.” Nature Metabolism 3(2):142–148.
Hales, C.M., M.D. Carroll, C.D. Fryar, and C.L. Ogden. 2020. “Prevalence of Obesity and Severe Obesity Among Adults.” U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics. Available online: https://www.cdc.gov/nchs/data/databriefs/db360-h.pdf (Accessed September 7, 2024).
Hernandez, I., D.R. Wright, J. Guo, and W.H. Shrank. 2024. “Medicare Part D Coverage of Anti-Obesity Medications: A Call for Forward-Looking Policy Reform. Journal of General Internal Medicine 39(2):306–308.
Kadouh, H., V. Chedid, H. Halawi, D.D. Burton, M.M. Clark, D. Khemani, A. Vella, A. Acosta, and M. Camilleri. 2020. “GLP-1 Analog Modulates Appetite, Taste Preference, Gut Hormones, and Regional Body Fat Stores in Adults with Obesity.” Journal of Clinical Endocrinology & Metabolism 105(5):1552–1563.
Kim, D.D., J.H. Hwang, and A.M. Fendrick. 2024. “Balancing Innovation and Affordability in Anti-obesity Medications: The Role of an Alternative Weight-maintenance Program.” Health Affairs Scholar 2(6).
Lincoff, A.M., K. Brown-Frandsen, H.M. Colhoun, J. Deanfield, S.S. Emerson, S. Esbjerg, S. Hardt-Lindberg, G.K. Hovingh, S.E. Kahn, R.F. Kushner, and I. Lingvay. 2023. “Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes.” New England Journal of Medicine 389(24):2221–2232.
Lipanovic, D. 2024. “GLP-1 Receptor Agonist Shortage Expected to Continue for All of 2024.” Pharmaceutical-journal.com, January 4. Available online: https://pharmaceutical-journal.com/article/news/glp-1-receptor-agonist-shortage-expected-to-continue-for-all-of-2024
Liu, B.Y., and B.N. Rome. 2024. “State Coverage and Reimbursement of Antiobesity Medications in Medicaid.” JAMA 331:1230–1231.
Liu, J., R. Micha, Y. Li, and D. Mozaffarian. 2021. “Trends in Food Sources and Diet Quality among US Children and Adults: 2003-2018.” JAMA Network Open 4(4):e215262.
Mansouri, J., and B.E. Roe. 2024. “Changes in Food Waste among a Sample of US Consumers after Beginning Anti-Obesity Medication.” Nutrients 16(19):3274.
Montero, A., G. Sparks, M. Presiado, and L. Hamel. 2024. “KFF Health Tracking Poll May 2024: The Public’s Use and Views of GLP-1 Drugs.” KFF, May 10. Available online : https://www.kff.org/health-costs/poll-finding/kff-health-tracking-poll-may-2024-the-publics-use-and-views-of-glp-1-drugs/
Novo Nordisk. 2024. “Updates about Wegovy®.” Available online: https://www.novonordisk-us.com/supply-update.html#wegovysupplychain [Accessed July 7, 2024]
Peck, E. 2023. “How Weight Loss Drugs Like Ozempic Could Radically Reshape the Food Business.” Axios, October 6. Available online: https://www.axios.com/2023/10/06/ozempic-weight-loss-drugs-food-business
Qeadan, F., A. McCunn, and B. Tingey. 2024. “The Association between Glucose‐Dependent Insulinotropic Polypeptide and/or Glucagon‐Like Peptide‐1 Receptor Agonist Prescriptions and Substance‐Related Outcomes in Patients with Opioid and Alcohol Use Disorders: A Real‐World Data Analysis. Addiction forthcoming.
Roe, B.E. (2024). “Anti-obesity Medication Patients’ Self-reported Food Savings versus the Cost of Such Medicines,” International Journal of Obesity, https://doi.org/10.1038/s41366-024-01708-y.
Rubino D., N. Abrahamsson, M. Davies, D. Hesse, F.L. Greenway, C. Jensen, I. Lingvay, O. Mosenzon, J. Rosenstock, M.A. Rubio, and G. Rudofsky. 2021. “Effect of Continued Weekly Subcutaneous Semaglutide vs Placebo on Weight Loss Maintenance in Adults with Overweight or Obesity: The STEP 4 Randomized Clinical Trial.” JAMA 325(14):1414–1425.
Scirica B.M., A.M. Lincoff, I. Lingvay, P. Bogdanski, S. Buscemi, H. Colhoun, A.E. Craciun, M. Ezhov, S. Hardt-Lindberg, O. Kleist Jeppesen, and A.L. Matos. 2024. “The Effect of Semaglutide on Mortality and COVID-19–Related Deaths: An Analysis from the SELECT Trial.” Journal of the American College of Cardiology 84(17):1632–1642.
Serafini, M., and E. Toti. 2016. “Unsustainability of Obesity: Metabolic Food Waste.” Frontiers in Nutrition 3:40.
Ward, A.S., B. Tysinger, P. Nguyen, D. Goldman, and D. Lakdawalla. 2023. “Benefits of Medicare Coverage for Weight Loss Drugs.” Schaeffer Center White Paper Series, University of Southern California. Available online at: https://healthpolicy.usc.edu/research/benefits-of-medicare-coverage-for-weight-loss-drugs/ (Accessed September 13, 2024)
Watkins, S., J.C. Toliver, N. Kim, S. Whitmire, and W.T. Garvey. 2022. “Economic Outcomes of Antiobesity Medication Use among Adults in the United States: A Retrospective Cohort Study.” Journal of Managed Care & Specialty Pharmacy 28(10):1066–1079.
Wharton, S., R.L. Batterham, M. Bhatta, S. Buscemi, L.N. Christensen, J.P. Frias, E. Jódar, K. Kandler, G. Rigas, T.A. Wadden, and W.T. Garvey. 2023. “Two‐Year Effect of Semaglutide 2.4 mg on Control of Eating in Adults with Overweight/Obesity: STEP 5.” Obesity 31(3):703–715.
World Health Organization (WHO). 2024. “Obesity and Overweight.” Fact Sheet. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (Accessed September 7, 2024).
Wreschnig, L.A. 2024. “Medicare Coverage of GLP-1 Drugs.” Congressional Research Service Report RF12758, Version 2, September 9. Available online: https://crsreports.congress.gov/product/pdf/IF/IF12758 (Accessed November 13, 2024).
Xu, F., K.Y. Wang, N. Wang, G. Li, and D. Liu. 2017. “Modified Human Glucagon-Like Peptide-1 (GLP-1) Produced in E. coli Has a Long-Acting Therapeutic Effect in Type 2 Diabetic Mice.” PLoS One 12(7):e0181939.

